Home | Yellow
Fever | Dengue | Japanese
encephalitis | Hepatitis C | West
Nile Virus
Dengue Virus
Profile
The Dengue virus is a member of the virus family Flaviviridae
and is transmitted to people through the bite of the mosquitos Aedes
aegypti and Aedes albopictus. Dengue virus is now
believed to be the most common arthropod-borne disease in the
world. Dengue is mainly found in the tropics because the
mosquitoes require a warm climate. A major fear of
epidemiologists is that the mosquitoes will develop resistance to
cooler climates and then be able to infect people in the United
States and other temperate climates. The virus is transmitted
when a mosquito of the Aedes genus bites an individual
infected with dengue virus. The virus in the blood of the
infected individual then infects the mosquito and travels from
the mosquito's stomach to its salivary glands were the virus
multiplies. The virus is then injected into another person when
the mosquito injects anticoagulants that prevent blood clotting
when the mosquito is feeding. The mosquito remains able to
transmit dengue for its entire life.
 Each year, 100 million people become infected
with dengue virus. People first reported the existence of dengue-like
disease in 1779 but it was most likely present long before in
first appeared in literature. However, the majority of deaths
that result from dengue infection result from Dengue Hemorrhagic
Fever (DHF) and Dengue Shock Syndrome (DSS). People who develop
DHF have a 5% chance of death but if they go on to develop DSS
then the mortality rate can rise as high as 40%.
Each year, 100 million people become infected
with dengue virus. People first reported the existence of dengue-like
disease in 1779 but it was most likely present long before in
first appeared in literature. However, the majority of deaths
that result from dengue infection result from Dengue Hemorrhagic
Fever (DHF) and Dengue Shock Syndrome (DSS). People who develop
DHF have a 5% chance of death but if they go on to develop DSS
then the mortality rate can rise as high as 40%.
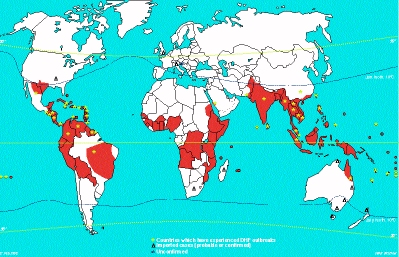
The General Distribution of
Dengue and/or Dengue Haemorragic
Fever, 1975-1998
The incubation period of dengue fever is approximately four
days. The person will come down with fever and present a discrete
macular or maculopapular rash. It is difficult to distinguish
dengue fever from other viral diseases and the person usually
recovers in 5 days. In more severe cases, fever and rash are
accompanied by headache, retroorbital pain, myalgia, backache,
sore throat, and abdominal pain. The patients become lethargic
and experience anorexia and nausea.
DHF has a similar incubation period as dengue fever and many
of the same symptoms. However, the fever is more severe and the
drowsiness and lethagry is more extreme. The patient has
increased vascular permeablilty and abnormal hemostasis. This can
cause the individual to lose blood volume, result in hypotension,
go into shock (DSS) and die.
 It is important to understand why an individual
will develop DHF/DSS. The Dengue virus has been shown to have 4
subtypes. These 4 subtypes are different strains of dengue virus
that have 60-80% homology between each other. The major
difference for humans lies in subtle differences in the surface
proteins of the different dengue subtypes. After a person is
infected with dengue, they develop an immune response to that
dengue subtype. The immune response produced specific antibodies
to that subtype's surface proteins that prevents the virus from
binding to macrophage cells (the target cell that dengue viruses
infect) and gaining entry. However, if another subtype of dengue
virus infects the individual, the virus will activate the immune
system to attack it as if it was the first subtype. The immune
system is tricked because the 4 subtypes have very similar
surface antigens. The antibodies bind to the surface proteins but
do not inactivate the virus. The immune response attracts
numerous macrophages, which the virus proceeds to infect because
it has not been inactivated. This situation is referred to as
Antibody-Dependent Enhancement (ADE) of a viral infection. This
makes the viral infection much more acute. The body releases
cytokines that cause the endothelial tissue to become permeable
which results in hemorrhagic fever and fluid loss from the blood
vessels.
It is important to understand why an individual
will develop DHF/DSS. The Dengue virus has been shown to have 4
subtypes. These 4 subtypes are different strains of dengue virus
that have 60-80% homology between each other. The major
difference for humans lies in subtle differences in the surface
proteins of the different dengue subtypes. After a person is
infected with dengue, they develop an immune response to that
dengue subtype. The immune response produced specific antibodies
to that subtype's surface proteins that prevents the virus from
binding to macrophage cells (the target cell that dengue viruses
infect) and gaining entry. However, if another subtype of dengue
virus infects the individual, the virus will activate the immune
system to attack it as if it was the first subtype. The immune
system is tricked because the 4 subtypes have very similar
surface antigens. The antibodies bind to the surface proteins but
do not inactivate the virus. The immune response attracts
numerous macrophages, which the virus proceeds to infect because
it has not been inactivated. This situation is referred to as
Antibody-Dependent Enhancement (ADE) of a viral infection. This
makes the viral infection much more acute. The body releases
cytokines that cause the endothelial tissue to become permeable
which results in hemorrhagic fever and fluid loss from the blood
vessels.
The most important aspect in treatment of DHF is to prevent
further fluid loss. Drugs such as corticosteroids or
carbazochrome sodium sulfonate are given to stabilize capillary
permeability and avoid plasma leakage. As regards to prevention,
a vaccine has proven rather difficult to produce. The reason for
this stems from the 4 subtypes of dengue. If an individual
develops immunity to one subtype and then tries to launch an
immune response to another subtype then they will develop DHF/DSS.
Work has been done on a tetravalent vaccine that will attempt to
give the individual immunity to all four of the subtypes at the
same time. Currently, the most effective prevention measures lie
in mosquito control.
References:
Kautner, Ingrid PhD; Robinson, Max MD; Kuhnle, Ursula MD.
"Dengue virus infection: Epidemiology, pathogenesis,
clinical presentation, diagnosis, and prevention." The
Journal of Pediatrics. Vol 131(4), October 1997, p 516-524.
Rigau-Perez, et al. "Dengue and dengue haemorrhagic fever"
The Lancet. Vol 352, Sept. 1998, p 971-977.