Project Description

Purpose
The treatment of patients with complex facial and neck trauma is one
of the most challenging multidisciplinary tasks in surgery. Simulation
technology based on 3D data of an individual patient will have a
critical impact on surgical planning and training. Repair of
maxillofacial fractures involves aligning fragments of bone with
accuracy so that aesthetics and function are restored. Surgery is
often lengthy and hindered by inability to fully view the fractures
from all angles due to anatomic difficulties such as muscular
attachments, vascular supply and critical nerve supply.
On-site and remotely accessible virtual environments capable of
simulating interactions with patient-specific anatomy will allow
surgeons to plan and rehearse operations and to retrain skills for
infrequent procedures. Selection of type of plate, its length,
alignment and screw length is currently done intraoperatively and
several alternatives might need to be considered in the operating
room. The ability to shift these decisions to a pre-operative planning
stage would decrease the length of surgery and improve confidence in
the accuracy of repair.
Commercially available maxillofacial surgery planning software allows
for interactive realignment of fractures based on segmented,
pre-operative CT images, but are limited to the interactions of
keyboard and mouse. This limited ability to control orientation of the
bone fragments and lack of force feedback on contact leads to low
perceived confidence of the resulting surgical plan.
Our goal is to overcome the limitations of current software by
designing and implementing a haptics-enabled maxillofacial surgery
rehearsal environment that requires little training and provides a
direct high-fidelity immersive experience for the operator. The system
would support six degree-of-freedom (6-DOF) haptic interaction for
bone fragments and plate alignment for pre-surgical planning to treat
mandibular fractures. Our aim is to evolve a design of real utility to
surgeons and, at the same time, ensure that it can be realized in
implementation by identifying and addressing the technological and
interaction design challenges through conceptual and technical
prototypes.
Methods
The design process has followed a user centered design method
concurrently with development of state-of-the-art collision detection
and haptic rendering algorithms. This dual process allows for
identification of requirements that may be met with currently
available technology as well as opportunities for improvements in
certain essential technological areas of particular value to this
project. The design is informed and iteratively improved by field
studies, lo-fi and hi-fi prototypes, scenarios and co-operative
evaluation with oral/maxillofacial surgeons.
During the design process we are iteratively implementing two main
prototypes, following the concepts of a vertical (few features, but
hi-fi interaction) and a horizontal (conceptually all features of the
system, but lo-fi interaction) prototype. The horizontal prototype
allows the surgeon to execute a typical usage scenario from beginning
to end. While not all features are fully implemented, and some may
only be mock-ups, the purpose of the horizontal prototype is to elicit
feedback and modify the prototype and scenario to identify the most
important aspects of the system. The risk with a horizontal-only
prototype is that the designer might use materials and technologies
that are infeasible or even impossible to implement. We balance this
risk with vertical prototypes that fully implement critical components
requiring new technologies, which act as proof of concept and informs
the overall design of what can be built.
One essential property of the rehearsal environment is the possibility
of bi-manual six degree of freedom positioning and orientation of
fractured mandibular bone in a way that looks and feels reassuring,
without requiring the user to learn a complex CAD-like system.
Real-time visualization of the dental occlusion and haptic feedback
conveying accurate contact forces while manipulating fractured bone
fragments are essential components of the system, and thus novel
technological development in these areas is required.
Results
The steps and interactions we identified include loading a segmented
CT-scan of a trauma patient, viewing it in a stereoscopic display
co-located with a bi-manual haptic interface, manipulating the bone
fragments, and perceptualizing the occlusion between maxilla and
mandible both visually and haptically through force-feedback. In
addition, the surgeon may lock the fragments into key positions, view
them from different directions, decide on plate placement and screw
sizes, and finally generate a report of the resulting surgical plan.
The form of our initial prototype was a pure mock-up (figure 1), and
was used as a conversation artifact to improve the design and build
common ground between surgeons and engineers.
Our studies indicate that the success of such a system is highly
dependent on the fidelity of the haptic rendering. For the rehearsal
environment to be intuitive, the interaction must follow the direct
intention of the operator with smooth and accurate force feedback. A
vertical prototype (figure 2) has been developed to focus on the
haptic rendering aspect of the system. It extends our group’s recent
work to formulate a new algorithm for rendering 6-DOF haptic
interaction between high-resolution volumetric representations of
objects (e.g. bone fragments from CT images). In addition to the
prototypes, we will report the results of an formative evaluative
study, which will include the grading of perceived usefulness and
fidelity of the interaction.
Conclusion
We show a maxillofacial surgery rehearsal environment that was developed
using an iterative design process with feedback from surgical specialists. The
system will permit surgeons to plan, simulate and rehearse complex repair of
maxillofacial fractures, including bone fragment and bone plate alignment in
three-dimensional space. The benefit of a haptics-enabled system for obtaining
accurate surgical results, reducing operating time, and for enabling a
platform to enhance surgical training in infrequent operations is considered.
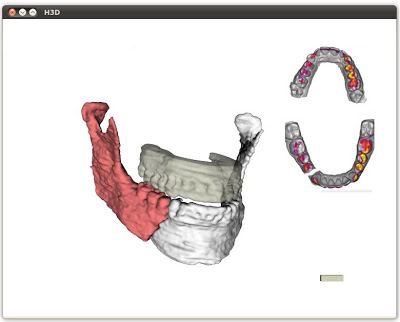
Figure 2. Screenshot from the interactive prototype. Each of the two
mandibular fracture segments can be moved with a left and a right haptic
device respectively.
Project Staff
Status
Active since 2010.
Funding Sources
Funded through VA Grant Number.