SITE CONTENT |
| GENERAL INFO | TAXONOMY | MORPHOLOGY | REPLICATION STRATEGY | VIRAL PROFILE |
| RECENT DEVELOPMENTS | DRUG PROFILES | PATHOGEN CARDS | LINKS | REFERENCES |
Paramyxoviruses are an important class of viruses which are associated with respiratory ailments, and common childhood diseases such as measles and mumps. Paramyxoviruses are a significant cause of morbidity and mortality globally, especially in children and the elderly.
| TAXONOMY |
| FAMILY: Paramyxoviridae | ||
| SUBFAMILY | GENUS | SPECIES |
| Paramyxovirinae | Paramyxovirus | Human Parainfluenza Virus type 1,3 |
| Paramyxovirinae | Rubulavirus | Human Parainfluenza Virus type 2, 4a, 4b , Mumps virus |
| Paramyxovirinae | Morbilivirus | Measles virus |
| Paramyxovirinae | Henipavirus | Hendravirus, Nipahvirus |
| Pneumovirinae | Pneumovirus | Respiratory Syncytial Virus |
| MORPHOLOGY |
Morphology
Paramyxoviruses encode negative-sense, single-stranded, monopartite RNA. They are enveloped and contain a helical nucleocapsid. They appear pleomorphic or spherical in electron micrographs.




| REPLICATION STRATEGY |
-ssRNA must first be converted into +ssRNA (mRNA) by the RNA-dependent RNA polymerase (RDRP) incorporated in the virion. The mRNA can then be translated into proteins. Replicative enzymes (RDRP) synthesize a negative-strand copy of the +RNA. Structural proteins translated from the mRNA are then used to package progeny -RNA and RDRP into virions.
| VIRAL PROFILES |
Measles
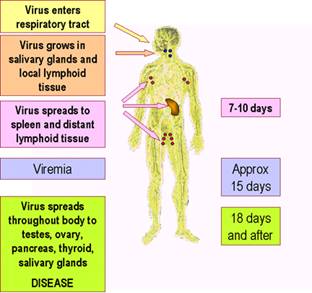
Incubation: Normally 8-14 days
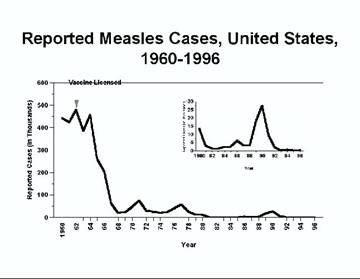
Epidemiology: There is only one serotype of measles that causes the disease. Main route of transmission is via inhalation. Recently the prevalence of measles has decreased dramatically in developed nations, but measles is still a problem in third-world nations, especially in Africa and Central and South America.
Symptomatology and Outcome

Oral exanthem of Measles infection

Classic non-vesicular exanthem associated with measles

Another classical case of measles exanthem
- Symptoms:
- Infected person first experiences fever, cough and runny nose. Occasionally includes conjunctivitis, or pink eye.
- Maculopapular rash normally appears 14 days into the illness. It starts at the head and moves down the neck to the lower part of the body and to the legs and arms.
- Koplik’s spots: Irregular, bright-red spots in mucosal membranes with bluish-white speck at center.
- Complications:
- Ear infections: most common complication (1/10 cases)
- Pneumonia: Very common complication and cause of mortality in developing countries. As many as 1/5 children with measles in developing countries can contract pneumonia.
- Diarrhea
- Post-infectious Measles Encephalitis:
- A complication from measles that leads to swelling of the brain that can be accompanied with meningitis. Proceeds from headache, fever and discomfort to loss of motor control, cognitive impairment, occasional seizures, visual loss and death.
- Can occur between 8 days and a month after infection.
- Occurs more commonly in children
- Sub-Sclerosing Panencephalitis, or SSPE
- A very rare complication from measles that is associated with a rare form of the virus
- Can arise anywhere from 1 to 12 years after initial measles infection
- Usually Fatal
- Symptoms progress from behavioral changes to loss of motor control and coordination, slurred speech, paralysis and eventually to death.
- Outcome:
- Most people who get measles normally recover. Serious complications, however, are more common in developing nations and in areas where access to healthcare and/or basic care is scarce.
- Measles is not normally deadly, but mortality and complications increase dramatically where malnutrition and vitamin A deficiency is common.

Prevention/ Management
- Vaccination with the Measles, Mumps and Rubella vaccine is very effective. Prevalence of Measles has significantly decreased in developed nations with successful vaccination programs
- Vaccine is currently administered in a 2-dose program at 12-15 months and again at 8-12 years of age.
- There have been a few adverse effects associated with vaccination, such as pneumonia and atypical measles.
- Treatment: there is no effective antiviral treatment or therapy for measles.
Mumps

Swollen parotid glands, a classic symptom of mumps
Incubation: 12-25 days, but normally 16-18 days
Epidemiology
Man is the only known natural host. Mumps is prevalent worldwide, but incidence has significantly decreased in developed nations due to MMR vaccination. Mumps is known as a “childhood” disease because it normally affects children under 10 years of age. The virus is transmitted by respiratory secretions and by saliva via aerosol form and/or fomites.
Symptomatology and Outcome
- Symptoms Include: fever, malaise, myalgia, anorexia and parotitis, or swelling of the parotid glands that causes the characteristic grimace appearance. Testicular inflammation, or orchitis, in males is another common symptom.
- Complications may include:
- Meningitis (15% of cases), which may include neck stiffness and
- Deafness (rare)
- Pancreatitis
- Myocarditis
- Joint pain and arthritis (most commonly in adult cases)
- Outcome:
- Complications are rare and most children fully recover after a few weeks

Prevention/ Management
-
The Measles, Mumps and Rubella vaccine has been very successful in decreasing the prevalence of Mumps.
-
The vaccine includes the three live-attenuated viruses. It is very effective (95% efficacy) and provides long term immunity.
-
There is no effective treatment for mumps except for treating symptoms such as fever and malaise in children by using analgesics and fever reducers.
Respiratory Syncytial Virus
Incubation: The incubation period of RSV is typically between 4 to 6 days.
Epidemiology
-
The most common cause of lower respiratory tract infections worldwide; Subtype A of RSV is the predominant infectious agent
-
Primarily a disease of the elderly and children
-
A leading cause of pneumonia and bronchiolitis in infants
-
Nearly all children are infected by age 2
-
Transmitted by the respiratory route
-
Infections occur mostly in the winter
Symptomatology and Outcome
- There are two sets of symptoms and outcomes
- Adults, and children age > 3.
- Congested or runny nose
- Dry cough
- Low grade fever, sore throat
- Mild headache, malaise
- Young Children
- High fever
- Severe cough
- Wheezing
- Rapid breathing
- Bluish skin color (cyanosis)
- May require hospitalization infants
Complications
-
Out of the 125,000 cases a year, a small percentage die, usually apnea or respiratory failure in young infants
-
RSV may be associated with Sudden Infant Death Syndrome (SIDS)
-
Otitis media
-
Brochiolitis, pneumonia
Outcome
- Most people quickly recover; usually within 8 to 15 days
Prevention/ Management
-
Treatment is mostly supportive, and includes hydration, and careful monitoring of respiratory status
-
Oxygen supplementation to ensure a 92% hemoglobin-oxygen saturation
-
Antibiotic therapy is given when secondary bacterial infections arise
-
Ribavirin is administered for 8 to 20 hours a day for 2 to 5 days in patients that are immunocompromised or have increased cardiac or pulmonary risk factors
-
Prevention is difficult, as the virus is readily transmitted by respiratory droplets
-
There is no vaccine for RSV
MYSTERIOUS ENCEPHALITIS IN BANGLADESH
In mid-January of 2004, there were ten deaths from encephalitis in Bangladesh. The culprit was found to be Nipah or a Nipah-like virus, Hendravirus, which is a recently discovered paramyxovirus. Nipahvirus is thought to have caused an encephalitis outbreak in 1998/1999 in Malaysia, resulting in 300 confirmed infections with 35% mortality rate. The virus is thought to be a zoonosis from pigs.
ACUTE RESPIRATORY INFECTION OUTBREAK IN CAMBODIA
Beginning on June 5, 2005, many children developed acute respiratory infections in Cambodia. Amongst the viruses detected were RSV, human metapneumovirus, parainfluenza viruses 1-4, and influenza A and B. Many of the cases were noted to be co-infections of RSV and influenza B.
DISCOVERY OF THE MODE OF NIPAHVIRUS CELL INFECTION
Scientists at UCLA have discovered how Nipahvirus, a virus that causes encephalitis and death in up to 70% of its victims, infects its host cell. The viral particle binds to Ephrin B-2, a receptor crucial to nervous system development and the growth of blood vessels.
DIFFERENTIAL RESPONSE OF DENDRITIC CELLS TO hMPV and RSV
Scientists at the University of Texas have recognized that dendritic cells respond differently to hMPV and RSV infection. Monocyte-derived cells were susceptible to infection by both viruses, but only RSV was able to effectively induce infection and replication of the viral particle. RSV-infected monocyte derived cells were more severely affected in their ability to stimulate CD4+ T cell production than hMPV infected cells. This research will allow scientists to create more effective medications to combat the different effects of each virus.
hMPV INDUCES A PROFILE OF LUNG CYTOKINES DISTINCT FROM THAT OF RESPIRATORY SYNCYTIAL VIRUS
hMPV induces differential cytokine production from RSV. This finding may bring about new potential treatments and/or establish new methodologies in diagnosis and differentiating between other respiratory tract infections.
Respigam (RSV-IGIV)
- Monoclonal antibody therapy
- Coat the virus, prevent viral binding to respiratory epithelial cells receptors
Palivizumab (Synagis)
- Another monoclonal antibody therapy
- Mode of action is similar to Respigam, but has less side effects
- Less hospitalization and adverse reactions reported
Proquad
- Measles, Mumps, Rubella, and Varicella Vaccine
- Administered between 10-12 months of age and 8 to 12 years of age
- Licensed for use in 2005

Jennifer Trayner's Excellent Site 1998
Leanna Brown 1999
Lisa Fleisher & Meagan Lansdale 2000
A Great Resource for Paramyxoviridae
Johns Hopkins RSV Information Page
Fields Virology.
Strauss, J. Viruses and Human Disease. Academic Press. December 2001.
Cann, A. "Paramyxoviruses." http://www.tulane.edu/~dmsander/WWW/335/Paramyxoviruses.html. Last updated 16 February 1999.
Sander, D. "All the Virology on the WWW." http://www.virology.net/garryfavweb13.html. Last updated 2004.
Sander, D. "The Big Picture Book of Viruses: Paramyxoviridae." http://www.virology.net/Big_Virology/BVRNApara.html
Microbiology and Immunology Online. “Measles and Mumps Viruses.”
November, 2004, http://pathmicro.med.sc.edu/mhunt/mump-meas.htm
CDC. “Measles: What you need to know.” 2005,
http://www.cdc.gov/nip/diseases/measles/vac-chart.htm
Anderson, J. The Morbillivirus Pages at the Institute for Animal Health. Last updated 1 March 1997.
The RSV Info Center. 2005. http://www.rsvinfo.com/sequelae/sequlae.html
Chen, CJ. Epidemiology of respiratory syncytial virus in children with lower respiratory tract infection. Acta Paediatr Taiwan. 2005 Mar-Apr; 46(2):72-6.
High, KP. Pneumonia in older adults. New categories add complexity to diagnosis and care. Postgrad Med. Oct 2005. (4):18-20, 25-8.
Wilmott, RW. Hoods are effective for aerosol delivery in RSV brochiolitis. J Pediatr. 2005 Nov; 147(5):A3.
Guerrero-Plata, A. Differential Response of Dendritic Cells to Human Metapneumovirus and Respiratory Syncytial Virus. Am J Respir Cell Mol Biol. 2005 Nov 11.
Null, D. Safety and immunogenicity of Palivizumab (Synagis) administered for two seasons. Pediatr Infect Dis J. 2005 Nov 24(11):1021-1023.
Questions or comments?
E-mail us: karu at stanford dot edu & urimanzo at stanford dot edu