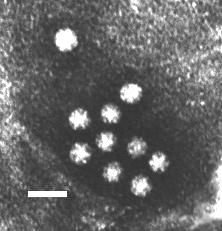
Stool sample from an individual with gastroenteritis.
Negative-stain Transmission Electron Microscopy. Bar = 50 nanometers.
F.P. Williams, U.S. EPA
Stool sample from an individual with gastroenteritis.
Negative-stain Transmission Electron Microscopy. Bar = 50 nanometers.
F.P. Williams, U.S. EPA
 Positive sense single-stranded RNA
(+ssRNA)NonenvelopedIcosahedral capsidSmall size (28-30 nanometers in diameter)Round viruses with characteristic starlike
surface appearance when viewed by electron microscopy, hence the name Astroviridae. Stars may be five-
or six-pointed.A ubiquitous virus, astrovirus infections are found
worldwide.Young children, especially in childcare settings, are most
likely to develop clinical illness.Elderly patients in nursing facilities and military recruits
have also experienced outbreaks of astroviral gastroenteritis. Astrovirus is an important cause of
enteric disease in immunocompromised individuals, too.Similar to rotavirus, astrovirus infections tend to occur
during winter months in temperate regions and in the rainy season in tropical regions.More refined detection techniques, such as reverse
transcription-polymerase chain reaction (RT-PCR), have demonstrated that astrovirus infection is more
common and important to viral gastroenteritis than previously shown.There is no vaccine for astrovirusPersonal hygiene and decontamination of outbreak settings
are important to reducing transmission and infectionIndividuals can continue to shed astrovirus in their feces several days
after illness resolves, and so should continue to take precautions after recovering from
overt illness.There is no anti-viral treatment for astrovirus infection,
and astroviral disease rarely requires hospitalizationHowever, young children who are at risk due to preexisting
malnutrition or illness should be treated with oral rehydration therapy (ORT) to avoid severe
consequences of gastroenteritis. ORT is also used for rotaviral infections and other diarrheal
diseases, such as cholera.Matsui SM, Greenberg HB. "Astroviruses." Chapter 28 in Fields
Virology, 4th edition. Fields B, Knipe D, Howley P, eds. Lippincott-Raven: Philadelphia, 2000
(875-893)The
Astrovirus Homepage of the Institute for Animal HealthICTV - International Committee on the Taxonomy
of VirusesAll the Virology on the WWW
Positive sense single-stranded RNA
(+ssRNA)NonenvelopedIcosahedral capsidSmall size (28-30 nanometers in diameter)Round viruses with characteristic starlike
surface appearance when viewed by electron microscopy, hence the name Astroviridae. Stars may be five-
or six-pointed.A ubiquitous virus, astrovirus infections are found
worldwide.Young children, especially in childcare settings, are most
likely to develop clinical illness.Elderly patients in nursing facilities and military recruits
have also experienced outbreaks of astroviral gastroenteritis. Astrovirus is an important cause of
enteric disease in immunocompromised individuals, too.Similar to rotavirus, astrovirus infections tend to occur
during winter months in temperate regions and in the rainy season in tropical regions.More refined detection techniques, such as reverse
transcription-polymerase chain reaction (RT-PCR), have demonstrated that astrovirus infection is more
common and important to viral gastroenteritis than previously shown.There is no vaccine for astrovirusPersonal hygiene and decontamination of outbreak settings
are important to reducing transmission and infectionIndividuals can continue to shed astrovirus in their feces several days
after illness resolves, and so should continue to take precautions after recovering from
overt illness.There is no anti-viral treatment for astrovirus infection,
and astroviral disease rarely requires hospitalizationHowever, young children who are at risk due to preexisting
malnutrition or illness should be treated with oral rehydration therapy (ORT) to avoid severe
consequences of gastroenteritis. ORT is also used for rotaviral infections and other diarrheal
diseases, such as cholera.Matsui SM, Greenberg HB. "Astroviruses." Chapter 28 in Fields
Virology, 4th edition. Fields B, Knipe D, Howley P, eds. Lippincott-Raven: Philadelphia, 2000
(875-893)The
Astrovirus Homepage of the Institute for Animal HealthICTV - International Committee on the Taxonomy
of VirusesAll the Virology on the WWW