1994 Project Reports | Contents | Previous | Next | Home |
Patient Handling: positioning and transfer of spinal cord injured patients
Eric E Sabelman, PhD; Charles Burgar, MD; Conal Wilmot, MD
Objectives - Safe movement of the human body is of primary concern to the high level spinal cord injured patient from the time of injury throughout his or her lifetime. The Rehab R&D Center has developed several devices in response to the short-term and long-range needs for effective patient handling equipment.
Appropriate handling of cervical spinal cord injured patients requires stabilization of the spine as the patient progresses through the early phases of rehabilitation. A Stabilization Transport System with integral backboard and constant force traction has been developed to reduce the risk of further injury during helicopter transport to a specialized spinal center and during routine nursing, therapy and diagnosis. An Active Positioning System with servo-controlled lateral support pads prevents relative motion of the patient's head and body during continuous side-to-side tilting on kinetic beds used to reduce the risk of pressure sores and respiratory or vascular complications. The goal is to develop a system capable of preventing the spine from shifting, while preventing pressure sore development.
 Figure
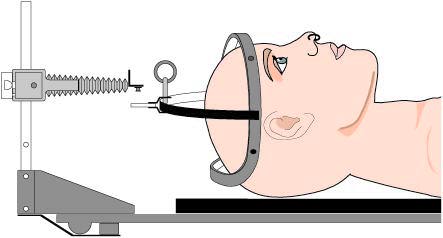
1. Constant force traction unit adapted to commercial backboard and halo.
Figure
1. Constant force traction unit adapted to commercial backboard and halo.
![]()
During long-term care, patients with insufficient upper limb function
need a lifting/transfer device to reduce their dependence on an attendant. The
objective of the Self-Operated Lift is to allow the disabled person to
independently move from bed to a wheelchair, and then to a car seat, bathtub or
toilet.
Approach - The development of the Stabilization Transport System began with the basic concept of a contoured radiolucent backboard with adjustable constant force traction. Enhancements include design of a lateral restraint pad, head and trunk straps, x-ray compatible skeletal fixation tongs and halos, and pre-production design of the traction device. The Stabilization Transport System has been laboratory tested against other commercial and experimental backboards for stiffness and ability to minimize relative body segment motion.
Kinetic beds commonly used for oscillating therapy of acute spinal injury patients provide insufficient restraint against movement of the patient's head relative to the body. The Active Positioning System includes a microcomputer that controls inflatable pillows located between the patient's body and the lateral restraint frame of the bed. If nonuniform motion of the head/trunk system is detected during tilting, the appropriate pillows are pressurized on the lower side of the patient to maintain head/trunk alignment. Pressure is released from the "uphill" pillows permitting sweat evaporation and restoration of skin blood flow.
A first prototype of the Self-Operated Lift was developed as a student project in the Stanford University's Mechanical Engineering Design Division to enable a quadriplegic to transfer between bed and wheelchair without the assistance of an attendant. The prototype featured a multiple tine surface for sliding under patients lying on a special air mattress with lateral inflatable tubes. Deflating every other tube provided access under the patient for the cushioned tines.
Status - Clinical usage of the Stabilization Transport System has been monitored since 1985, with no adverse effects. The Stanford/Life-Flight team continues to fly all its spinal cord injured patients using the Stabilization Transport System. Work on this project has led to a search for objective methods for evaluating its efficacy under realistic dynamic conditions, motivating a pilot study of accelerometric measurement of relative head-to-body motion during routine patient handling procedures. Efforts are underway to commercialize the traction unit either as part of the Stabilization Transport System, or adapted to other commercially available beds and spineboards. The traction unit has also been incorporated into a resistive exercise device for small hand muscles.
An initial mock-up of the Active Positioning System has been constructed to compare water-inflatable pads with conventional fixed lateral pads, using a simulated bed and body mass (sand bag) instead of an actual patient. Water is pumped from the "uphill" pads to the lower pads as the bed tilts and non- uniform motion is detected. Test runs with passive (foam) pads and active pads have been videotaped with reflective markers on the bed and simulated body for computer motion analysis.
Initial tests with normal subjects on the Self-Operated Lift found deficiencies sufficient to require a major redesign. However, the multiple tine approach was particularly well suited for beds having deep air cushions with the tines sliding between the cushions without deflation. Improvements to be incorporated on the next version include attention to frictional problems between the patient and tines, hinging the back section closer to the hip center, and addition of a foot rest and side rails. An alternative concept consists of a combined lifting and conveying mechanism.
Republished from the 1994 Rehabilitation R&D Center Progress Report. For
current information about this project, contact
Eric Sabelman.